METHODOLOGY
Intensive Short-Term Dynamic Psychotherapy (ISTDP)
As its name indicates, ISTDP is a model of dynamic psychotherapy, since it is based on the principles of Sigmund Freud’s Psychoanalysis and Melanie Klein’s Object Relations Theory. However, it differs substantially both from standard psychoanalysis, as well as from psychoanalytic psychotherapy. One of the main differences is that the psychotherapist is particularly active and persistent during sessions, in an attempt to aid the patients in overcoming their resistance and experiencing their emotions. ISTDP is also a short-term type of therapy, as it may last from one up to forty sessions, while standard psychoanalysis and psychoanalytic psychotherapy would perhaps require several years to reach completion. ISTDP is intensive because it involves significant activation of the patient on behalf of the therapist, as mentioned above.
Aside from the psychodynamic theory, the concepts and theories of emotional trauma and attachment or bond (Attachment theory). According to Attachment theory, in order to develop emotionally in a normal manner, a child requires a close relationship with a so-called primary carer, who tends to be the mother. It may, however, more seldom also be the father, a grandmother or an older sibling, or a nursery teacher. These carers must be emotionally mature themselves (as the paediatrician and psychoanalyst Donald Winnicott says, a “good enough mother”) so that the child to successfully incorporate all the emotional provisions, to construct and organise their ego and to feel capable of forming relationships with themselves and others in a mature and comprehensible way, experiencing their feelings without undue anxiety (Image 1).
Creation of Mental Disorders-Symptoms


However, due to the various stimuli that the child or adult is exposed in daily life later, these feelings tend to resurface, rising inside the child or adult intense anxiety and developing behaviours that affect both the calmness and consistency of the self, as well as the individual’s relationships with other persons, hence causing some or more psychopathological symptomatology (Image 2).
The aims of ISTDP
The goals of Intensive Short-Term Dynamic Psychotherapy are to enable the patient to experience all of their repressed emotions that are frequently triggered and cause distress, while simultaneously fostering structural changes in their character and personality. This is achieved by increasing their capacity to tolerate the anxiety elicited by their emotions, as well as helping them feel better about themselves and others, thereby improving their interpersonal relationships. The goal of ISTDP is for the patient to succeed in experiencing all of their repressed, frequently activated and disruptive emotions, while simultaneously to bring about structural changes to their character and personality, as the anxiety that the emotions invoke becomes more bearable and the patient begins to feel better towards themselves and others, which results in improved relationships. This of course will also positively affect both performance and relationships at work. Likewise, the patient is now more capable of receiving satisfaction and joy from activities and entertainment. Essentially, the therapy aims to restore the primary childhood bond that had been ruptured. (Image 3).
The Punitive Judge
Often, what pushes the patient into suffering and behaving in a self-destructive way is a part of their psyche which the psychodynamic theory terms as “superego” and which we could, in lay person terms, liken to a strict and particularly punitive judge. We all have this judge inside of us, but there are different types of judges. Some are particularly lenient and humane, some incorruptible, while others are punitive and bloodthirsty. We create and develop the inner judge from the moment we are born, and his function is to help us control our aggressive and erotic drives and feelings so that we can coexist harmoniously within society. Unfortunately, when our feelings of anger and rage from our childhood are particularly intense or even murderous, the superego takes on the form of this particularly controlling and punitive judge, in order to control them. This results in the person having a rather restricted psyche and developing a depressive and self-punishing attitude towards life.
In practice, during the therapy the judge will attempt to push the patient into resisting the therapist and patient’s joint efforts for change towards a more humane and carefree life. Therefore, early in the therapy the patient should be encouraged and aided in facing this judge and converting him to a more benevolent supervising force.
Anxiety and its forms
As is widely known, anxiety is a natural neuro-chemical-hormonal physical process which aims at arming the individual with energy and the ability to react to an upcoming danger or irritation or demand of the environment. The person experiences this process mentally and physically.
For several reasons, every person has a natural ability to bear a certain level of rise in their anxiety. The muscular system manifests this natural expression of anxiety in the form of tension. When this anxiety is intense or chronic it may cause the person to experience tremors, fatigue or chronic muscular pain (backache, neck pain, fibromyalgia)
Among individuals, however, who experienced significant and frequent emotional trauma during infancy or childhood, there are cases where anxiety – rather than being directed towards and experienced into the striated/voluntary muscles – is directed towards and experienced into the viscera and most frequently the stomach or the intestines or the respiratory airways or blood vessels. Those are comprised from muscular fiber of a different type (involuntary lean muscle). The result is that the individual experiencing anxiety into the viscera may suffer from stomach aches, gastritis, psychogenic peptic ulceration or frequent diarrhoea or constipation, asthma or psychogenic hypertension or migraines.
In other individuals with an even higher level of rise in anxiety, or lesser ability to tolerate anxiety, this may affect their ability to concentrate or even the function of their vision or hearing, or more rarely also their other senses, resulting in the individual experiencing fuzziness or disorganization of thinking or even ceasing of thinking, as well as blurry vision or central vision with blurry peripheral vision or also tinnitus or temporary hearing loss.
It is not surprising that these individuals struggle considerably in their daily lives when their anxiety rises, and as a result experience discomfort and may also be rendered significantly dysfunctional. Another repercussion is that, when they enter therapy, whether ISTDP or not, their anxiety rises, causing the above issues and rendering them unable to function well and productively. This hinders the therapy from progressing and yielding the expected results.
Therefore, for such individuals there is a pressing and primary need to learn to withstand and regulate their anxiety. In ISTDP, the therapist learns to observe and control the patient’s anxiety levels from the start and to help them experience it exclusively into the striated muscles and not the viscera or the brain. In other words, the therapist helps the patient build up their capacity to bear even a high rise in their anxiety, without manifesting the above pathology.
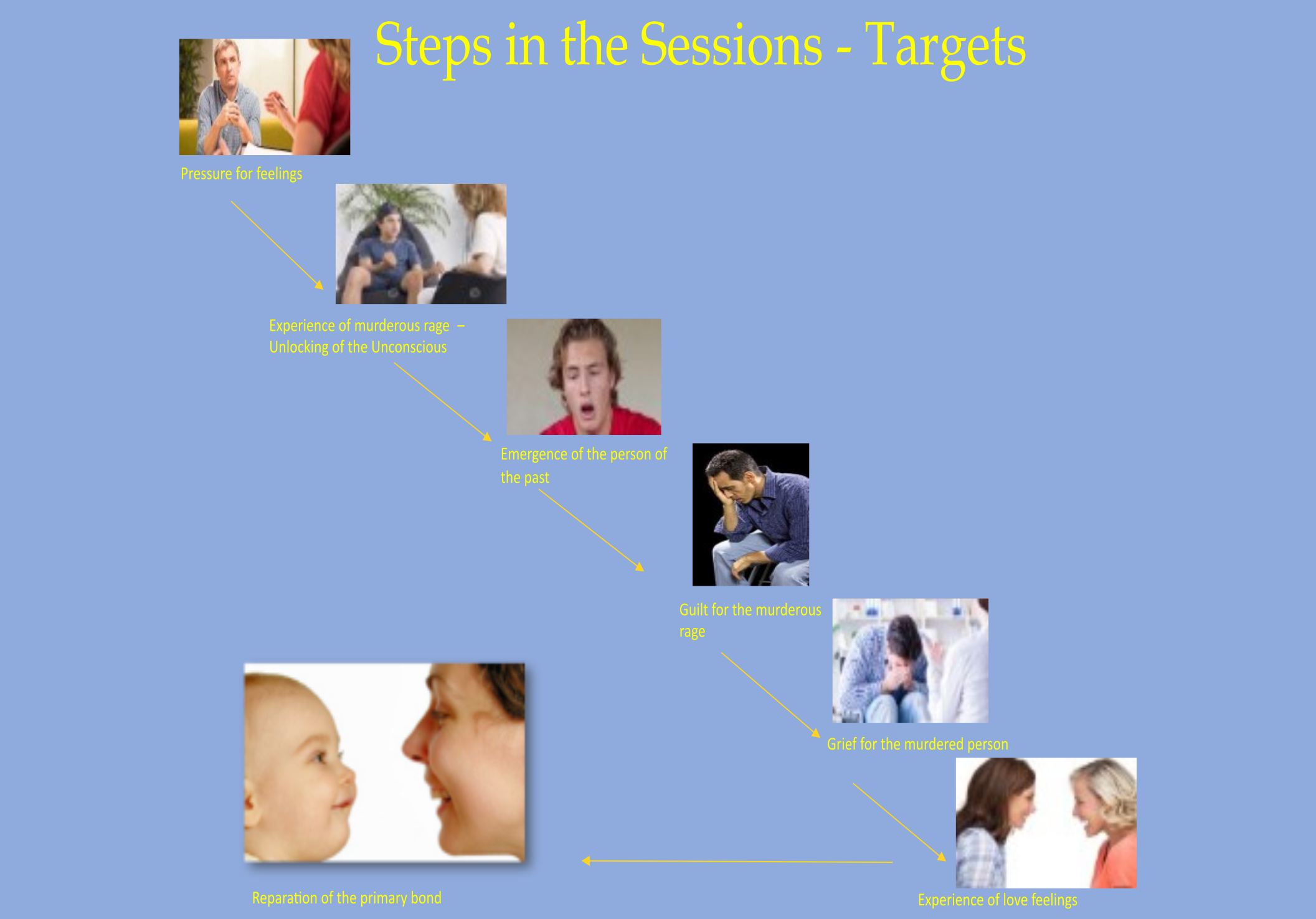
Experiencing the repressed feelings - Unlocking the unconscious
As mentioned above, the therapist and therapy itself share the goal of helping the patient experience all the feelings they had experienced during childhood due to the trauma that they underwent, while at the same time also to comprehend the reasons why those feelings were formed and how they affected the patient, leading to pathological behaviours and physical symptoms. This normally starts with experiencing the feelings that arise in the patient’s everyday relationships, as well as in the relationship with the therapist. Usually, following this type of experiencing in the here and now, the patient recognises the face of the person from the past who traumatised them in that of the therapist or the person from their present life. In this way, they will then experience the repressed feelings they hold towards the person or persons of the past. This is what is called the unlocking of the unconscious and the emergence of repressed/hidden material. This experiential and mental process has a profound effect on the patient’s issues and behaviour. It must be repeated multiple times during the therapy, depending on how much the patient was traumatised during childhood.
Patient resistance to the therapeutic process
In ISTDP, as has been mentioned previously, the patient must experience all the feelings that were repressed during childhood. In order to achieve this, the therapist will press the patient in this direction, starting from the relationships of the present and the therapist-patient relationship.
As the emergence of the feelings from the unconscious is a relatively painful process and as the punitive superego/judge resists every effort for the betterment of the patient’s life, wanting to constantly punish them or to control their negative feelings towards their loved ones, the patient will begin to resist the therapist’s pressure to experience the feelings. The obstacles the patient puts in the therapist’s way are in psychotherapy terms called defences and their function is referred to as resistance to therapy.
Therefore, an important task for the therapist is to point out to the patients the obstacles they themselves put in the way and how destructive these are for the therapy and their life itself, and then to ask them to set those obstacles aside. This effort on behalf of the therapist, particularly during the first few sessions, is a considerably demanding and tiresome process. However, if the therapist remains consistent in pressing for the defences to be abandoned and the feelings to be experienced, in the end, both the therapist and the patient will be rewarded by a beautiful collaborative relationship which leads to the resolution of the patient’s issues.
ISTDP therapy duration
As said previously, the duration of ISTDP ranges from one to forty sessions. Davanloo himself defined this limit, stating that after 40 sessions the therapy should be considered long-term. Of course, there exist cases that may require more than 40 sessions. In this case, we could argue that this therapy is an extended version of psychoanalytic therapy, but with elements of ISTDP.
Which mental disorders or issues can ISTDP address?
ISTDP can be applied on and prove effective for more than 90% of the cases that seek help at a psychiatric practice. More specifically, it can be applied on:
- Mood disorders such as depression or dysthymia. It may also be applied to cases of manic-depressive or bipolar disorder, which are, however, regulated and not in a phase of mania or hypomania. In such cases, ISTDP may help reduce relapses, as well as medication and dosage.
- Stress related and somatoform disorders, such as generalised anxiety disorder, panic disorder with or without agoraphobia, social phobia, individual phobias, obsessive-compulsive disorder, Post Traumatic Stress Disorder (PTSD), dissociative (conversion) disorders such as hysteria, somatoform disorders such as the so-called psychosomatic disorders, hypochondriasis etc.
- Personality disorders such as borderline personality disorder, narcissistic, histrionic, avoidant personality disorder etc.
- Eating disorders such as psychogenic anorexia and bulimia, and finally
- Medically regulated and stabilised psychosis, always, however, ensuring that the anxiety does not rise too high. In such cases, ISTDP may help reduce relapses as well as the number and doses of medication and to make the patient more functional.
Contraindications for ISTDP
Patients experiencing active psychosis, mania, or hypomania should not be treated with Intensive Short-Term Dynamic Psychotherapy (ISTDP). Furthermore, patients with severe Antisocial (Psychopathic) Personality Disorder are excluded from this treatment. Additionally, patients with severe functional or autoimmune diseases—such as Crohn’s disease, ulcerative colitis, or severe asthma—should not be treated with ISTDP while in an acute phase (exacerbation), nor should patients with severe angina. Finally, patients using “hard drugs” cannot be treated with ISTDP during periods of systematic use.